Lacrimal System Infections
Dacryoadenitis
- Symptoms include pain, tenderness and swelling of the lateral aspect of the eyelid
- May occur with systemic diseases such as Sjogren's, sarcoidosis, syphilis, TB, lymphoma, and benign lymphoid hyperplasia
- May occur in patients with mums, EBV, zoster
Canaliculitis
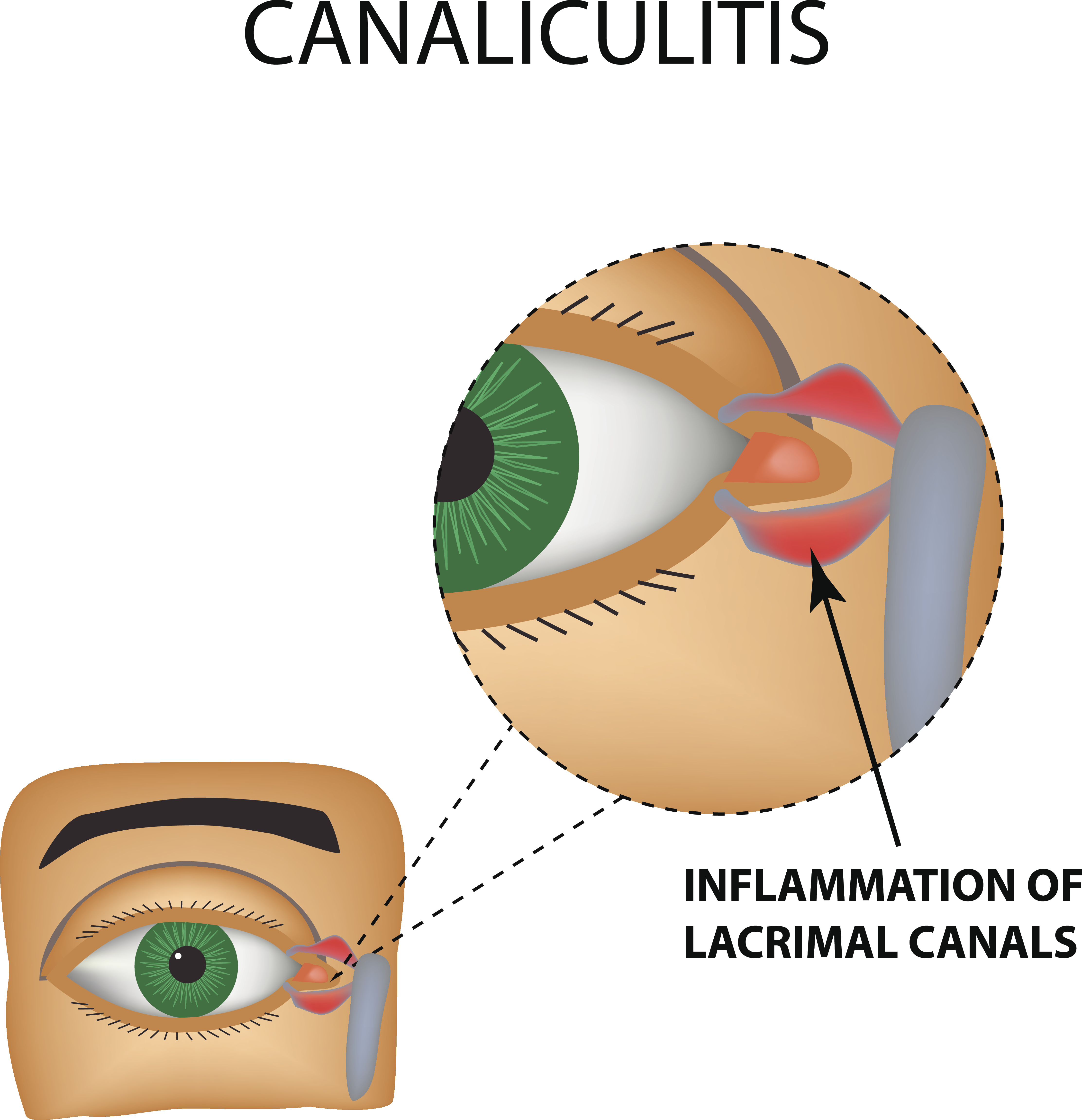
- Canaliculitis is a clinical condition that is characterized by infection of the canaliculi in the eye. It commonly affects individuals over the age of 50 years. It is caused due to obstruction within the canaliculus, the presence of a foreign body or the presence of diverticulum which harbours bacteria within it.
Pathophysiology of canaliculitis
As has been mentioned above, canaliculitis occurs due to infection of the canaliculi. This infection is often brought on by bacteria though there could be alternative aetiology such as fungi and viruses as well. The most common cause of canaliculitis is Actinomyces Israelii. However, the other causes can include aspergillus, Canada albicans and even herpes simplex and herpes zoster virus.
Infection by these organisms results in the formation of tiny stones that are rich in sulphur. These stones form little pockets that unfortunately are not affected by the antimicrobial properties of tears.
History and examination
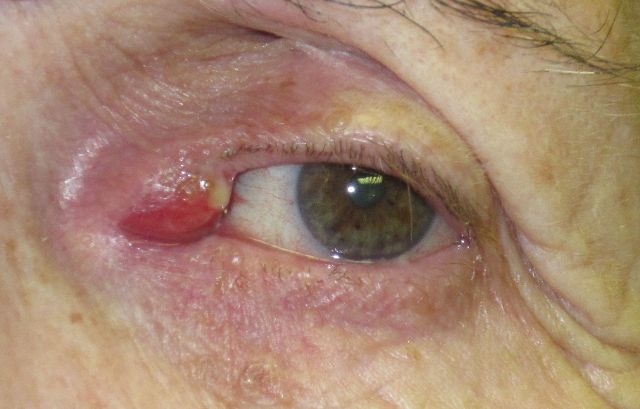
Patients often complain of a long-standing history of one eye being red and inflamed. The inner aspect of the eye constantly displays a thick discharge which can be clear or rather discoloured.
On examination, the lacrimal punctum is swollen and inflamed. The swelling is due to accumulation of fluid and is called oedema. The area is tender to touch. When gently compressed, the cloudy, purulent discharge is expressed through the punctum.
Diagnosis is through clinical history and examination in most cases. If a probe is passed through the lacrimal punctum, a grating sensation is experienced due to the presence of sulphur stones (concretions) within it.
Laboratory investigations are conducted on the discharge. Tests are conducted to ascertain the type of infection that is affecting the canaliculus. Staining could be performed with a different stains and microscopic assessment could reveal the presence of organisms such as Actinomyces or aspergillus.
Treatment
- The treatment of canaliculitis is fairly straightforward and involves the application of warm compressions, massage of the local area and antibiotic creams and ointments applied locally. These treatments could or could not help the patient. In the event of this being the case, patients could require to undergo a surgical procedure to help clear the infection. This is usually offered when irrigation with a sterile solution and broad-spectrum antibiotics is ineffective. Procedures can include deployment of the canaliculus through a procedure called canaliculotomy.
- The procedure is fairly straightforward and is performed by making a tiny incision on the conjunctival aspect of the canaliculus. The sulphur concretions are then removed and antibiotics are used to clear any residual infection.
Conclusion
- Canaliculitis is a rare condition that affects individuals over the age of 50 years. It is characterised by bacterial or fungal infections within the canaliculi and the formation of concretions that are rich in sulphur. Treatments can include topical antibiotics and drainage, though in some cases surgical treatment could be required.
- Symptoms include pain, swelling, tenderness of the INNER canthus of the eye
- Etiology is usually actinomycetes
Dacryocystitis
- Symptoms: acute onset, tearing (from nasolacrimal duct obstruction), redness, purulent discharge, tender swollen lacrimal sac
- An infection within the "tear duct" causes a painful swelling in the inner corner of the eyelids.
- If the tearing causes severe symptoms, surgery can be performed to create a new tear duct. This operation is called "dacryocystorhinostomy." (see below). Small silicone tubes my be placed in the tear system to keep the new tear duct open while healing occurs. Surgical elimination of the obstruction by creating a new tear duct is necessary to eliminate the tearing and infection that can result from such a blockage
Acute Dacryocystitis

- various etiologies, all cause nasolacrimal duct obstruction with obstruction of drainage from lacrimal sac to nose
- chronic tear stasis causes 2o infxn
- edema, erythema below medial canthal tendon w/lac sac distention
- +/- pain
- rule out ethmoidal sinusitis, don't probe
- Treatment
- warm compresses
- oral/IV abx (Keflex, Augmentin), topical only limited value
- Incision Drainage localized abscess
- Complications
- mucocele, chronic conjunctivitis, orbital cellulitis
- most need DCR after acute infection subsides

Chronic Dacryocystitis
- distended lac sac with minimal inflammation suppurative discharge from punctum c/w nasolacrimal duct obstruction
- probe/irrigate upper system only
- dacryoliths from Actinomyces, Candida, topical meds, can cause lacrimal colic if impacted in NLD
- Treatment usually needs DCR for resolution
Lacrimal Fistula

